Joint strategic needs assessment
Health and Homelessness (2019)
This is an online synopsis of the topic which shows the executive summary and key contacts sections. To view the full document, please download it.
| Topic title | Health and Homelessness (2019) |
|---|---|
| Topic owner | Homeless Executive Steering Group |
| Topic author(s) | John Sheil, Susan March, Nick Romilly & Dawn Jenkin |
| Topic quality reviewed | September 2019 |
| Topic endorsed by | Homeless Executive Steering Group |
| Topic approved by | Health and Wellbeing Board November 2019 |
| Linked JSNA topics |
|
Executive summary
 Download infographic as PDF
Download infographic as PDF
Introduction
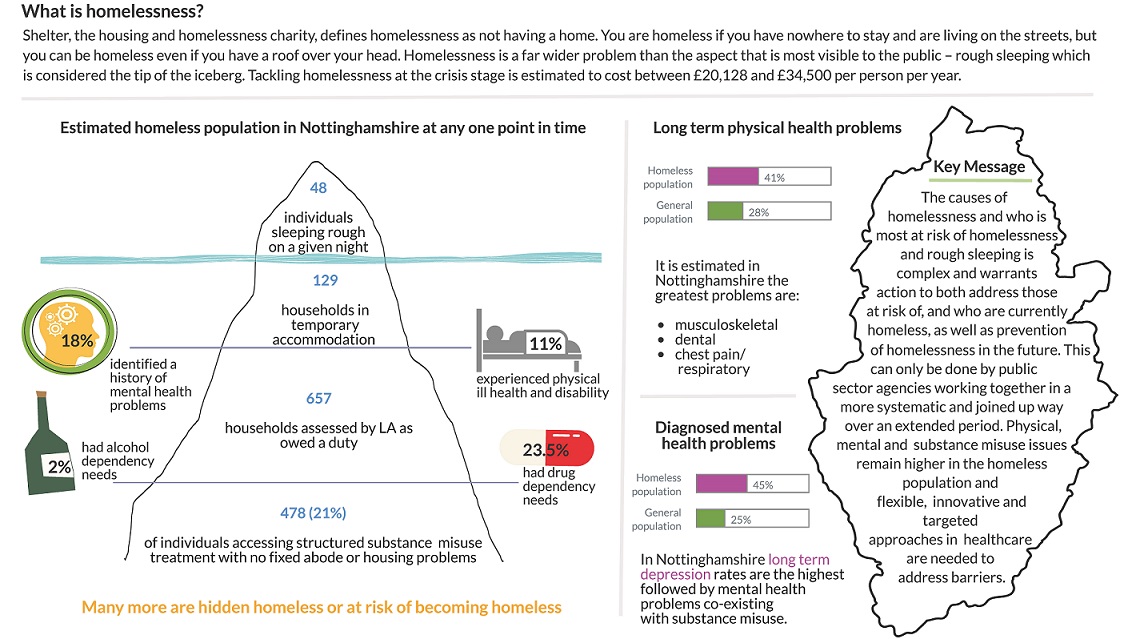
Shelter defines homelessness as not having a home[i]. You are homeless if you have nowhere to stay and are living on the streets, but you can be homeless even if you have a roof over your head. You count as homeless if you are:
- staying with friends or family
- staying in a hostel, night shelter or B&B
- squatting (because you have no legal right to stay)
- at risk of violence or abuse in your home
- living in poor conditions that affect your health
- living apart from your family because you don't have a place to live together
Homelessness is an issue of concern across the country and Nottinghamshire is not exempt from this picture. Homelessness is a far wider a problem than the aspect that is most visible to the public – rough sleeping which is considered the tip of the iceberg[ii].
The causes of homelessness and who is most at risk of homelessness and rough sleeping is complex and warrants action to both address those that are at risk of and who are currently homeless as well as attention to how we can prevent homelessness in the future. This can only be done by agencies from across the public sector working together in a more systematic and joined up way over an extended period.
People who are homeless experience worse health outcomes than the general population. Consequently, the focus of this JSNA chapter is on the physical and mental health needs of the homeless population as well as identifying who is at greatest risk of becoming homeless, the causes of homelessness and evidence of what works to prevent homelessness and respond to homelessness when it arises.
This JSNA chapter was endorsed by the Homeless Executive Steering Group with additional feedback provided by local organisations that formed the JSNA steering group or contributed towards the local views section. Whilst this JSNA chapter does not replace any previous version it does provide a more up to date narrative on the health and wellbeing of those who are homeless than the Assessment of the impact of housing on health and wellbeing (2013) JSNA chapter and builds on the 2013 assessment of the Health Needs of Single Homeless People in Nottinghamshire.
Unmet needs and service gaps
Housing and health need in Nottinghamshire must be set in the context that levels of statutory homelessness and rough sleeping remain low in the County and well below the England average. However, rough sleeping numbers have shown a steady increase since 2010, with variation across districts and boroughs, and higher rates occurring in Mansfield and Bassetlaw. This gives an indication of a rising level of unmet health, social, welfare or housing need.
Housing supply and welfare
This JSNA has highlighted a number of factors that are known to affect availability of affordable and appropriate housing, in particular for the most vulnerable populations at risk of homelessness due to complex needs and debt arrears. Specific issues highlighted within this JSNA include
- Lack of affordable housing
- Housing benefit set at rates lower than landlord can obtain in rent on the open market
- Private landlords unwilling to consider housing people in receipt of benefits
- Private rental barriers to housing people aged under 35 years
- Need for support in tenancy to prevent eviction
- Housing options to support people with experience of homelessness and existing rent arrears
- Recent trend in increased use of bed and breakfast accommodation in some areas within Nottinghamshire
Whilst approaches to address housing supply in these cases are critically important to securing positive outcomes and reducing homelessness, these are rightly covered within the Homelessness Strategies produced by local Housing Authorities. Therefore, the recommendations of this JSNA will focus on the non-housing risk factors leading to homelessness and how these wider needs can be met.
It is clearly acknowledged that neither housing approaches nor wider health and social care support can be truly effective in isolation to prevent homelessness. These needs are interconnected and therefore implementing effective solutions requires dedicated and strongly aligned partnership working.
Primary prevention approaches
The role of upstream primary prevention initiatives is not yet fully understood or embedded within strategic approaches, either nationally or locally. This is likely driven by, amongst other factors:
- The need to focus limited local resources on addressing the most acute and immediate needs of those at risk of homelessness
- The diffuse and system wide nature of risk factors leading to homelessness
It is recognised that a range of local provision which commissioners currently invest in has the potential to significantly contribute to the prevention of poor outcomes through homelessness. These include, but are not limited to:
- Debt, tenancy sustainment and welfare advice
- Veteran support strategies
- Housing adaptations secured through disabled facilities grant
- Substance misuse services
- Domestic abuse and sexual violence support services
- Family mediation
- Coping and resilience approaches in school settings
- Improving Access to Psychological Therapies (IAPT), talking therapies, social prescribing and befriending initiatives
- Employment support
- Ex-offender support strategies
It is difficult and possibly counter productive to identify unmet need in any single preventative approach, in particular as evidence points to the fact that those at risk of homelessness are far from a homogenous cohort and benefit from personalised approaches taking into account a range of support needs.
The opportunity across existing primary prevention approaches is for commissioners and providers to recognise that housing plays a critical role in health and wellbeing outcomes, and the services they provide have additional benefits of reducing future risk of homelessness. Strong joint working across services alongside improved awareness and skills in considering the housing needs of clients has the potential to maximise health outcomes for clients with complex needs within existing resource. The “duty to refer” introduced in the Homelessness Reduction Act provides an opportunity to engage a wider frontline workforce on the impact of housing on health and identify needs earlier.
Early Intervention and support
Consultation with local stakeholders showed a perception that support where available was not well known about, nor readily accessible. There was also a perception that support was not offered early enough and did not cover the broad range of the needs experienced by service users. Whilst the introduction of the Homelessness Reduction Act may address the need for earlier identification and support to some extent, consideration needs to be given to how support offers can be made more visible and accessible. In particular, for individuals who experience complex needs or chaotic lifestyles consideration needs to be given to targeted or tailored outreach approaches which reduce the barriers to engaging with services for support, in order to reduce the risk of exclusion and worsening health inequalities.
Services and commissioners may also need to consider how the profile of available support can be raised in frontline settings, to facilitate a “no wrong front door” approach to support at the point of care.
Governance and leadership
The wide range of services which have a role in supporting better health outcomes for those at risk of homelessness means that strong governance and leadership is needed at strategic level, to drive, support and hold to account effective delivery across a partnership. Stakeholders have described current partnership arrangements as operational rather than strategic, which may limit effectiveness to drive system change such as strategic commissioning of care pathway approaches. The Rough Sleeping Strategy suggests the introduction of Homelessness Reduction Boards which would take on the role of leading system change.
Healthcare
Users of homeless services locally have reported particular barriers to accessing healthcare appointments and mental health services. This can be considered in the context that national evidence shows individuals who are rough sleeping or in temporary accommodation are high users of healthcare. The combination of difficulties accessing care, with high levels of health need (mental and physical) leads to high volume service use for potentially preventable conditions. In order to better meet the healthcare needs of this population, flexible, innovative and targeted approaches are needed which specifically address the barriers presented by having no fixed abode, no access to transport, multiple health needs and in some cases chaotic lifestyles. Some examples of such innovative practice have been piloted in primary and secondary care settings in Nottinghamshire but are not as yet commissioned in line with population need in an integrated approach. Given the relatively small numbers of individuals who present with high levels of complex need or in crisis (as compared to the population as a whole), a targeted approach, delivered in settings most accessible to homeless individuals, with high levels of support and case management, is most likely to be effective in meeting need. Effectiveness is likely to be enhanced by delivery alongside providers with existing trusted relationships in homeless communities.
This JSNA highlights that substance misuse, musculoskeletal (MSK), dental and respiratory problems are likely to be the most prevalent physical health needs, along with a broad range of presenting common and severe mental health conditions. In addition, homeless populations face inequalities in access to screening programmes for both communicable and non-communicable conditions. Inclusion health standards highlight that providing equitable care in this population requires opportunistic approaches to offer screening and treatment.
Integrated commissioning and care pathways
Both service users and commissioners have reflected that commissioned support appears fragmented, potentially duplicative, and in some cases with lack of clarity as to thresholds and eligibility criteria. Where service users present with multiple or complex needs this can result in multiple assessments, referrals and delays in care, which in a worst-case scenario leads to disengagement by the service user and difficulty in supporting recovery within temporary accommodation settings. One strategy to support service users in navigating care is the use of a case worker, however it is unclear whether case worker capacity is sufficient to meet existing needs, and fragmented care pathways will also impact on the effectiveness of case workers themselves.
The service gaps particularly noted include management of support for those with mental health and/or social care needs, although interactions between all services are perceived as challenging.
Therefore, there is a critical need for commissioners (together with providers) to work jointly in creating effective care pathways which will deliver better value for individual services through more efficient processes, and better outcomes for service users through joined up person centred approaches.
The evidence base suggests that care-pathways designed around critical time intervention, identifying high risk groups at specific points, such as discharge from prison or other institution can offer an effective risk stratified approach. Examples of such approaches are currently being trialled as part of the Rapid Rehousing Pathway, providing navigators for prisons, hospitals and mental health services. To maximise the opportunities for effectiveness in these pilots, specific partner commitment is needed for:
- Robust evaluation and sharing of learning across the local system
- Development of integrated care pathways which address wider health and social needs in addition to housing provision
- Development of sustainable financial investment to embed effective practice emerging from the pilot
Knowledge gaps
This JSNA has relied on a combination of local views, local commissioned research and national data to develop a picture of health needs for those at risk of homelessness. There is very little reliable local data available to allow robust assessment of the scale of homelessness and the range of local health need.
This is a gap mirrored at national level and highlighted in the Rough Sleeping Strategy. Further work is needed for commissioners and providers to routinely collate and share information locally on the risk factors and health, housing and social care needs of those accessing services, as a starting point for estimating true population health need. It is expected that the new Homelessness Case Level Information Collection (H-CLIC) data will provide some useful data to better quantify need in those owed a support duty.
Recommendations for consideration by commissioners
| Recommendation | Lead(s) | ||
|---|---|---|---|
Strategic Leadership, Governance and Partnership Working |
|||
| 1. |
Establish formal governance arrangements in line with Ministry of Housing, Communities and Local Government (MHCLG) proposals for a Homelessness Reduction Board, to provide leadership and accountability for improving health and homelessness outcomes, including delivery of JSNA recommendations. |
Housing Authorities, Commissioners of Supported Housing |
|
| 2. |
Establish a coordinated or integrated strategic commissioning forum to address gaps in provision and enable effective care pathways across housing, social care, mental health and primary and secondary healthcare. |
Housing Authorities, Supported Housing Commissioners, Clinical Commissioning Group (CCG), Adult and Children’s Social Care |
|
| 3. |
Identify opportunities through the Homelessness Strategies of Nottinghamshire Housing Authorities to support prevention and early identification of homelessness by partners across the system, including best use of duty to refer. |
Housing Authorities |
|
| 4. |
Consider the recommendation of the Rough Sleeping Strategy that strategic leadership is provided through a dedicated Homelessness lead on the Health and Wellbeing Board. |
Health and Wellbeing Board |
|
Integrated Commissioning and Care Pathways |
|||
| 5. |
Develop and implement a commissioned care pathway for critical time intervention with specific high-risk groups: ex-offenders, mental health needs, veterans, substance misuse. |
Strategic Commissioning Forum |
|
| 6. |
Identify opportunities to align funding to evidence based primary prevention of homelessness, including through family mediation, debt advice, healthy lifestyles, tenancy sustainment initiatives, and education/support in at risk groups. |
Homelessness Reduction Board |
|
| 7. |
Develop the healthcare offer across primary, secondary and community care to meet the specific health needs of those with no fixed abode or in temporary accommodation, in line with inclusion health standards. |
CCG, Health Care Providers |
|
| 8. |
Identify opportunities to strengthen effectiveness of Street Outreach and Rapid Rehousing Pathway initiatives through system wide engagement, pathway development and advocacy for longer term funding settlements. |
Homelessness Reduction Board |
|
| 9. |
Identify and implement strategies for opportunistic screening and treatment for communicable diseases including blood borne viruses and tuberculosis, in settings most accessible to at risk homeless populations. |
Public Health England (PHE), Health Protection Strategic Group, CCG |
|
Implementation - Service Models, evaluation and data collation |
|||
| 10. |
Embed evidence based psychological approaches to managing and recovering from complex trauma into front line delivery of service, including Psychologically Informed Environments and trauma informed services (ReACH) |
Service Providers |
|
| 11. |
Develop robust and shared methods for data collation and evaluation for existing services, to improve local knowledge of risk factors and health needs for those at risk of homelessness |
Strategic Commissioning Forum |
|
| 12. |
Develop a strategic assessment of the Housing First model, as an option for securing long term health and social gains for individuals with complex and enduring needs, including substance misuse. |
Strategic Commissioning Forum |
|
| 13. |
Develop shared protocols across service provision to improve accessibility and visibility of early identification and support options. |
Service Providers |
|
[i] Shelter https://england.shelter.org.uk/housing_advice/homelessness/rules/what_is_homelessness accessed 3.7.19
[ii] LGiU (June 2019) LGiU Homelessness Commission 2019: Final Report https://www.lgiu.org.uk/wp-content/uploads/2019/06/LGiU-Homelessness-Commission-Final-Report.pdfaccessed Sept 2019
Key contacts
This is an online synopsis of the topic which shows the executive summary and key contacts sections. To view the full document, please download it.